
The Gulf Under Fire: How the US–Iran War Is Reshaping Regional Healthcare

Photo by UX Gun on Unsplash
The conflict that began on February 28, 2026 has already claimed lives in every Gulf Cooperation Council (GCC) member state. But the casualty count — twelve dead in the UAE, six in Kuwait, three each in Bahrain and Oman, two in Saudi Arabia, sixteen injured in Qatar — is the easiest part of this crisis to quantify. Harder to measure, and in many ways more consequential, are the slow-burn health effects that will outlast the shooting by decades.
This analysis draws on field reporting current to April 9, 2026. It traces the arc from direct injuries and infrastructure collapse through to the longer environmental and psychological toll, and it closes with what Gulf health systems are actually doing in response.
When Hospitals Lost Power
Iranian retaliatory strikes on Gulf energy grids have done something that no regional planner had fully stress-tested: they forced hospitals to choose, in real time, between keeping the lights on and keeping patients alive. Non-emergency surgeries have been suspended across multiple facilities. Life-support equipment has switched to backup power — where backup power exists.
The damage is not just structural. Shockwaves from nearby explosions have cracked windows in clinical areas, disrupted sterile fields, and caused staff to shelter rather than treat. The psychological cost to frontline workers — people who trained to manage disease, not war — has not yet been reported systematically, but it will be.
The Logistics Collapse: $26 Million in Limbo
Dubai’s WHO global health emergencies logistics hub — one of the world’s critical nodes for humanitarian medical supply — is effectively frozen. Airspace closures and Strait of Hormuz cargo restrictions have blocked $18 million in humanitarian health supplies and stranded another $8 million already in transit. More than fifty emergency supply requests from twenty-five countries are stuck in the backlog, among them medicines for Gaza and polio laboratory supplies. At least 1.5 million people across the region are downstream of this blockage.
The WHO, UNICEF, and World Food Programme are rerouting through alternative hubs and overland channels. This takes longer and costs more. For insulin-dependent patients or those mid-way through chemotherapy, “longer” is a clinical variable.
Freight insurance premiums for vessels transiting the Strait of Hormuz have surged by more than 1,000 per cent since late February 2026 — a figure that was already double what it had been before the Houthi escalation in 2024. Generic drug prices will follow the freight index upward. They always do.
Toxic Fallout: The Contamination That Will Outlast the War
Strikes on oil installations and fuel depots are releasing a toxic mixture that the Gulf region is only beginning to reckon with. Microscopic soot particulates raise the long-term risk of cardiac and pulmonary disease. Toxic chemicals from burning fuel infrastructure introduce cancer risk. Heavy metals from missile debris settle into soil and sediment, contaminating water supplies at a level of persistence that no clean-up programme has ever fully reversed in a comparable conflict zone.
Oily, acidic rain — soot and ash combining with atmospheric moisture — is falling back to earth across downwind areas. This is not a new phenomenon in Gulf conflicts, but the scale and the proximity to dense urban and industrial populations gives it a particular urgency here.
The GCC’s near-total dependence on desalinated water makes this worse. Desalination plants are vulnerable to both direct strike and to marine pollution from sunken vessels — oil and toxic residue can clog intake systems or require costly shutdown. Any prolonged disruption to desalination is, without exaggeration, an existential risk to urban populations in a region where groundwater is negligible. Secondary infectious disease outbreaks — cholera, hepatitis — become a real prospect when sanitation systems lose reliable water.
Ras Laffan and the Global MRI Supply Chain
The March 18 strike on Ras Laffan deserves its own section because its global health implications extend far beyond the Gulf. Qatar’s Ras Laffan is the world’s single largest source of helium — a gas that remains essential for cooling the superconducting magnets in most MRI scanners. The market was already volatile; the strike has introduced genuine supply uncertainty.
There are approximately 50,000 MRI machines in service worldwide, with 5,000 new units produced each year, and more than 95 million MRI scans performed annually. Prolonged helium scarcity will increase prices, delay procurement cycles, and put particular pressure on systems in lower-income countries that have less buffer stock and fewer alternatives. The clinical ripple from a missile strike in Qatar will eventually be felt in a radiology department in Lagos or Karachi.
The Psychological Toll: 30–50 % Under Acute Stress
Between 30 and 50 per cent of populations in directly exposed areas are reporting symptoms consistent with acute stress disorder, post-traumatic stress, or clinical anxiety. Sleep disturbance and emotional exhaustion are widespread. This is not just a consequence of direct proximity to strikes; prolonged exposure to war-related media and the low-frequency threat of an attack that may or may not materialise generates its own chronic stress load.
Gulf mental health services were not dimensioned for this. They were built for a peacetime population with peacetime referral pathways. The demand curve has changed faster than the service infrastructure.
The Nuclear Dimension: A Risk That Cannot Be Modelled Away
One stated aim of the US–Israeli operation is to eliminate Iran’s nuclear weapons capability. Strikes on enrichment facilities have already occurred, and Iran has retaliated with missile attacks on Israeli towns, including one housing a nuclear research centre. The health consequences of a radiological release — skin damage, radiation sickness in the short term; cancer, cardiovascular disease, and genetic damage across generations — are well-documented from previous incidents. What is less discussed is that even a non-detonation attack on a nuclear facility can scatter radioactive material across a wide area.
Gulf health ministries have no historical playbook for this. Their emergency protocols were written for petrochemical incidents, not radiological ones.
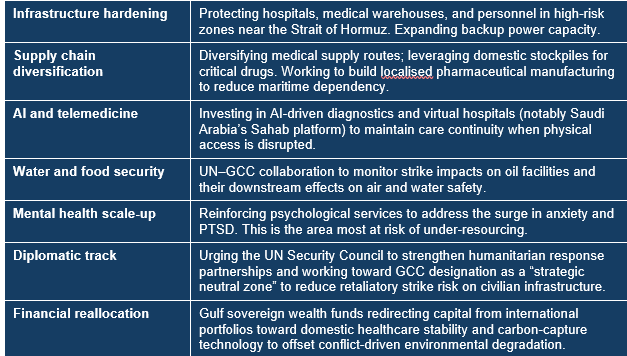
What the GCC Is Doing About It
The Gulf Health Strategy 2026–2030, originally conceived for a peacetime improvement agenda, has been pivoted in real time toward conflict resilience. The shift is captured in a phrase the GCC health ministers are now using repeatedly: “predictive, personalized, and preventive” — but built to survive an attack, not just a pandemic.
Conclusion: A Test of Health System Resilience, Not Just Geopolitics
The US–Israel–Iran conflict is testing something that no audit has ever fully examined: whether modern, technology-rich Gulf health systems can absorb the simultaneous shock of infrastructure damage, supply chain collapse, environmental contamination, mass psychological trauma, and the shadow of radiological risk — all at once.
The honest answer, so far, is: partially. The investment in AI, telemedicine, and strategic stockpiling represents genuine institutional learning. The gaps — mental health capacity, water infrastructure protection, radiological emergency planning — are real and not yet closed.
The global public-health community should not treat this as someone else’s regional problem. The WHO logistics paralysis in Dubai, the helium shortage rippling toward MRI suites worldwide, the generic drug price inflation that will follow the freight premium spike — these are everyone’s problems. Rapid coordination now, before the backlog becomes a backlog of preventable deaths, is what distinguishes a health system from a collection of hospitals.
References
1. Amadiume N, Boyce N. Environmental consequences of armed conflict: a review for policy and practice. Global Environmental Change. 2019;60:102003.
2. Baranes G, Fiske G. Health impacts of urban conflict: a systematic review. Lancet Glob Health. 2016;4(10):e677–e688.
3. Brown O, Crawford A. The environment and conflict: a primer for policy-makers. London: Chatham House; 2009.
Doctor Dialogues | May 2026 | All rights reserved