
War on the Ward: Gulf Healthcare Before, During, and After the US–Iran Conflict

Photo by Alexandr Popadin on Unsplash
The US–Israel confrontation with Iran, and its spillover into Gulf Cooperation Council (GCC) territory, is generating a public-health emergency with at least three distinct layers: the immediate trauma of injury and infrastructure damage; the medium-term collapse of supply chains and disease surveillance; and the long-term burden of environmental contamination, displaced populations, and psychological injury. None of these layers resolves before the next one deepens.
This analysis examines each layer in sequence — first the state of Gulf healthcare before the conflict, then the acute impacts and what health systems should be doing about them, and finally what a credible path forward looks like. The picture is serious. It is not hopeless.
Gulf Healthcare Before the Conflict: A System Mid-Transformation
It matters where a health system starts when war finds it. The GCC was not starting from weakness.
In the five years to March 2026, the Gulf recorded nearly 400 healthcare investment transactions, with Saudi Arabia and the UAE accounting for roughly 92 per cent of activity. Capital moved across the full care spectrum — acute hospitals, digital health platforms, outpatient and home care, rehabilitation, long-term care, and pharmaceutical manufacturing. In early 2026, over US$33 billion in new agreements was announced, a 125 per cent increase on 2024 levels. [1]
The numbers behind that investment are substantial. GCC hospital beds reached 127,600 — an average of 20.8 per 10,000 population, above the global average — with 73 per cent in government facilities. Primary and specialist health centres numbered approximately 3,400 across the region. The healthcare workforce stood at 1.05 million professionals, growing at 6.8 per cent annually: around 203,100 physicians, 78,700 pharmacists, and 411,900 nursing personnel. [1]
Saudi Arabia’s Vision 2030 is the most visible driver of this transformation. It targets privatisation of 290 hospitals and 2,300 primary health centres, with private sector involvement rising from 40 to 65 per cent of healthcare delivery by 2030. The 2025 health and social development budget was $69.3 billion — the second-largest share of Saudi government spending. The 2026 budget, approved in December 2025, maintained that commitment while tightening efficiency across all sectors.
The direction of travel across the GCC — toward predictive, personalised, preventive care underpinned by AI and digital infrastructure — had been consistent for a decade. The conflict has not reversed that direction. It has, however, violently complicated the journey.
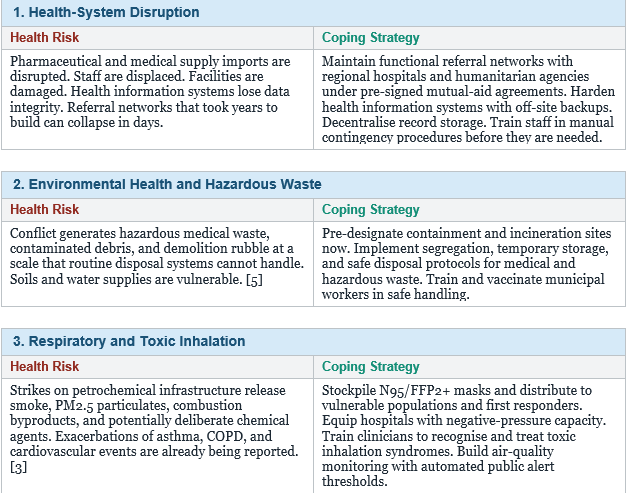
The Immediate Impact: Ten Threats Health Systems Must Confront Now
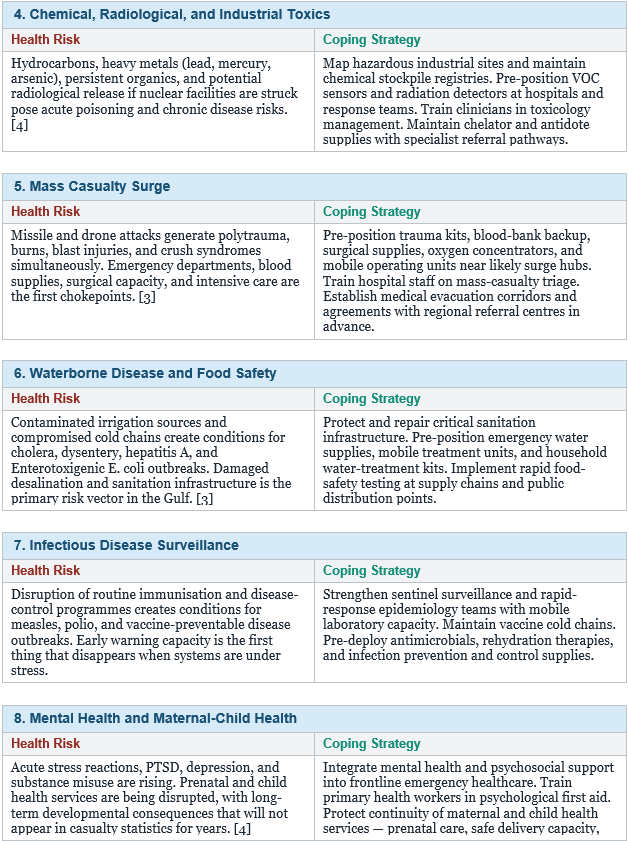
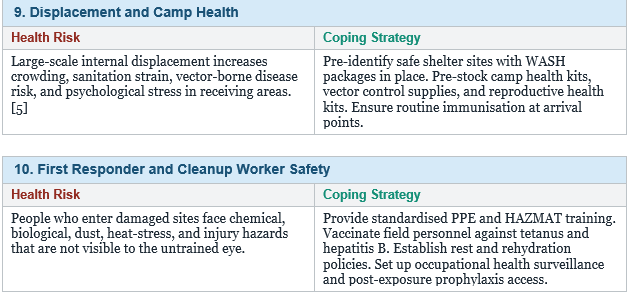
The following threats are not theoretical. All are already materialising to varying degrees across GCC states. For each, the evidence on what works — and what must be pre-positioned before the window closes — is reasonably clear.
Two Cross-Cutting Requirements
Two issues cut across every threat above and are often the first casualties of emergency improvisation.
Risk communication is not a public-relations function. When misinformation fills the vacuum left by official silence, health behaviours deteriorate faster than disease spreads. Pre-approved multilingual messaging, trusted spokesperson networks, and channels that work without internet — radio, SMS, community leaders — need to exist before the emergency, not be assembled during it.
Reliable data and legal documentation are the foundation of accountability. Standardised collection of clinical and environmental exposure data — through registries, with samples preserved — is what makes later health assessments and compensation claims possible. Lack of data does not mean the harm did not occur. It means it cannot be proven.
Equity is the third cross-cutting issue. Children, the elderly, people with disabilities, internally displaced persons, and women face disproportionate health risks and face more barriers to services. Any allocation of medical resources that does not account for this will systematically miss the people most in need.
The Way Forward: What a Credible Global Response Looks Like
The WHO is coordinating health responses across affected countries, supporting ministries and partners to sustain essential services, strengthen disease surveillance, pre-position trauma supplies and essential medicines, and scale readiness for chemical, biological, radiological, and nuclear risks. The honest assessment is that these operations face a serious funding gap. Without urgent financial support, essential services will not merely slow down — they will cease. Preventable suffering will deepen. [6]
The GCC’s own Gulf Health Strategy 2026–2030, originally designed for a peacetime improvement agenda, is being adapted in real time for a conflict environment. That adaptation deserves international support, not just acknowledgment.
Long-term recovery planning cannot wait for the conflict to end. Cancer registries, neurodevelopmental follow-up programmes, and chronic respiratory disease surveillance need to be designed now, while the baseline data still exists to make them meaningful. Post-conflict health monitoring is not a luxury. It is the mechanism by which a health system learns what it needs to repair.
Conclusion
The public-health consequences of the US–Iran conflict for GCC countries are going to be multifaceted and prolonged. That is not a counsel of despair — it is a call to specificity. Supply prepositioning, surveillance enhancement, health system hardening, targeted protection for vulnerable populations, and disciplined risk communication can each substantially reduce mortality and long-term morbidity. They require decisions and resources now, not after the next wave of casualties makes the need undeniable.
The Gulf health systems that stood at the frontier of regional ambition in early 2026 are the same systems that will carry the burden of recovery. Protecting their capacity — their staff, their data, their supply lines, their infrastructure — is not a strategic afterthought. It is the work.
References
1. Healthcare at the Crosshairs of Crisis in War Zones. HealthcareAsia.org, 2025. https://www.healthcareasia.org/2025/healthcare-at-the-crosshairs-of-crisis-in-war-zones
2. BMJ on war and healthcare systems. BMJ. 2025;389:r1320. https://www.bmj.com/content/389/bmj.r1320
3. Amadiume N, Boyce N. Environmental consequences of armed conflict: a review for policy and practice. Global Environmental Change. 2019;60:102003.
4. Haines A, Scheelbeek P, Abbasi K, et al. Health effects of environmental disasters from conflict: a call for preparedness. Lancet Planet Health. 2020;4(9):e375–e376.
5. Kloos H, Ustun TB. Public health in conflict settings: principles and practice. Bull World Health Organ. 2018;96(11):760–831.
6. World Health Organization. Health in emergencies: public health risk assessment and management in conflict-affected settings. WHO Technical Guidance; 2015.
Doctor Dialogues | May 2026 | All rights reserved